Oh no! You were scheduled multiple 4 hours shifts. Or worse, you floated for 4 hours, and floated for another 4 hours, with report putting that down to 3 hours (minusing your break). How do you optimize workflow and get everything done and know what you are doing? Don't fret.
1) Look at the patients. Do a quick scan. Then rapid fire quick scan of their chart: Look for abnormal labs, Pending procedures, Diet, Code status, Vitals.
2) Quick assess: Mental status, IV Site, Airway, Drips running, Drains, pain, and skin assessment.
3) Cluster EVERYTHING. This is key. Cluster all your meds passes, fluids, glucose, assessment, Emptying drains, repositioning, vitals if needed. Do not return to pt's room unless necessary. On a 4 hour shift your goal is to be a task monkey and prioritiziation. This is not the time for customer service, getting warm blankets, and getting snacks, or getting stuck in patient rooms. Delegate more due to time limitations.
4) Deal with your disaster patient first before your shift spirals. Pain, behavioral, confused fall risk, etc.
5) Chart immediately after each room. Your brain is fastest when info is fresh.
6) Accept that some things won't get done. No time for long conversations with patients, deep chart review, whiteboards, blankets, non-urgent care tasks. Focus on meds, assessment, safety, acute changes, and documentation.
7) Utilize relief nurse. IV out? Don't even try. You don't have time. Get relief nurse to help with labs and IV's.
8) Walk into the room knowing already what to do: Assessment, flush IV, meds.

You've only been a nurse for 1 year and they've assigned you as relief nurse. You're afraid of not knowing what to do and the ambiguity of this role. You must now think big-picture. You're uncomfortable without structure, but this entry will serve as a guide to giving "structure" to your role as relief nurse.
First, what does being a relief nurse require? You need big-picture awareness of the whole unit, delegation clarity, and rapid prioritization across multiple assignments. How do you gain big-picture awareness of the unit? Think about: Who is unstable? Who’s about to admit? Are labs pending? Any teles going wild? Staffing issues? Who needs help? Who’s drowning but won’t say it?
During chart review, ask yourself: "Wait, who has the admit?", "What’s the plan for that lactate?", "Did anyone call about bed 12?", "What do I even prioritize right now?"
You are there to see what others can’t see (big picture), prevent small problems from becoming RRTs, support flow, protect the most overwhelmed nurse on the floor
DO NOT: Hover awkwardly, Insert yourself into every room, Be everyone’s extra pair of hands all at once, read minds.
- Relief RN Structure:
- 1) For the first 30 min, check: Any high lactates? Any fresh admits? Any pending transfers? Anyone on restraints? Anyone refusing care? Any tele patients with weird rhythms? Any blood hanging or due? You don’t deep dive every chart. Just scan for instability. You’re hunting for: "Who could blow up in the next 2 hours?"
- 2) Walk the unit physically: Look at rooms, listen to tones, notice agitation, notice which nurse looks overwhelmed. If you do help, offer targeted help. Instead of: "Do you need anything?" Say: "Do you want me to grab vitals in 12?" "I can hang that antibiotic for you." "Want me to answer that call?" "I can sit with 8 while you chart." Specific offers make you look confident.
- 3) Always track: Admits coming up, transfers out, unstable labs, staffing gaps
- 4) For downtime, start doing relief duties and chores:
- Assign Vocera's, help with Admit/Transfer/Discharge, assign break of RN’s, FAX assignments to CMR (0730/1530/1930/2330), fill-up Med Carts & tidy hallway (put away beds, bladder scan, translator, IV carts and etc.), refill gloves for Room 05 – 39.
- Tidy clinical integration room, order N95 mask PRN check ALL cassette medications for right patient and expiration date/label. CHG audit (if applicable), glucometer QC, insulin inventory, smoke check for AIRBORNE rooms, check crash carts
- Massimo check admission/DC rooms, environmental check on DC rooms, ensure RNs signed the TELE strips, sign off Narcotic sheet & Equipment count & TELE BOX count (0730/1530/2330)and do narcotic counts (Mondays).
One of the bedside RN's just called an RRT on one of their patients. You're relief. You're expected to intervene and assist. What do you do? Let's bring structure to chaos. As a relief nurse, your role during a RRT is extremely valuable. The bedside nurse is focused on the patient; you become the unit stabilizer and logistics coordinator.
1) Immediately go to the room. Your first job is to quickly assess the scene. Ask the bedside nurse one question: “What’s going on?” You only need the 10-second summary: Example: “He desatted to 78%.” “BP suddenly 70/40.” “New stroke symptoms.” “He collapsed.” This tells you which direction the situation is going.
2) Take over the room logistics. The bedside nurse should stay with the patient. You help with everything else. Immediately check: Monitoring → Ensure telemetry attached, pulse ox waveform good, BP cycling every 2–3 min. Oxygen → Check if oxygen actually connected? Is flow turned up? Is mask fitted correctly? Access Do they have an IV? Is it working? If not → get supplies ready.
3) Clear the room. RRT rooms become chaotic. Your job is to control the environment.
4) Prepare for what the RRT will need. Equipment: Crash cart outside room, Suction Setup, Yankauer ready, Ambu bag, Extra oxygen mask, Non-rebreather. Supplies:IV start kit, Flushes, saline bag, pressure bag, lab tubes, EKG leads.
5) While the bedside nurse is tied up, their other patients still exist. You should: Cover their call lights, give their scheduled meds if needed, answer alarms, update the charge nurse if more help is needed. Think: “How do I protect the rest of the unit while this is happening?”
6) When RRT or MD arrives, the bedside nurse will give SBAR. You help by filling in missing information if needed. Example things you may know: Recent labs, Recent vitals, What meds were just given, Baseline mental status.
7)Assist with tasks: Starting an IV, drawing labs, hanging fluids, getting an EKG, getting supplies, running specimens. You become extra hands.
8) Watch for patient deterioration. Notice things like: Patient becoming lethargic, work of breathing worsening, telemetry changes, BP crashing. If something changes, say it out loud to keep the team aware.
9) Prepare for possible transfer. Many RRTs end with ICU transfer. You can start preparing: Patient chart ready, transport monitor, gather belongings, call report assistance if needed.
10) After RRT, recheck other patients.
Focus on environment, equipment, and workflow.
- ACCESSORY Kit: Open and set-up on top of cart
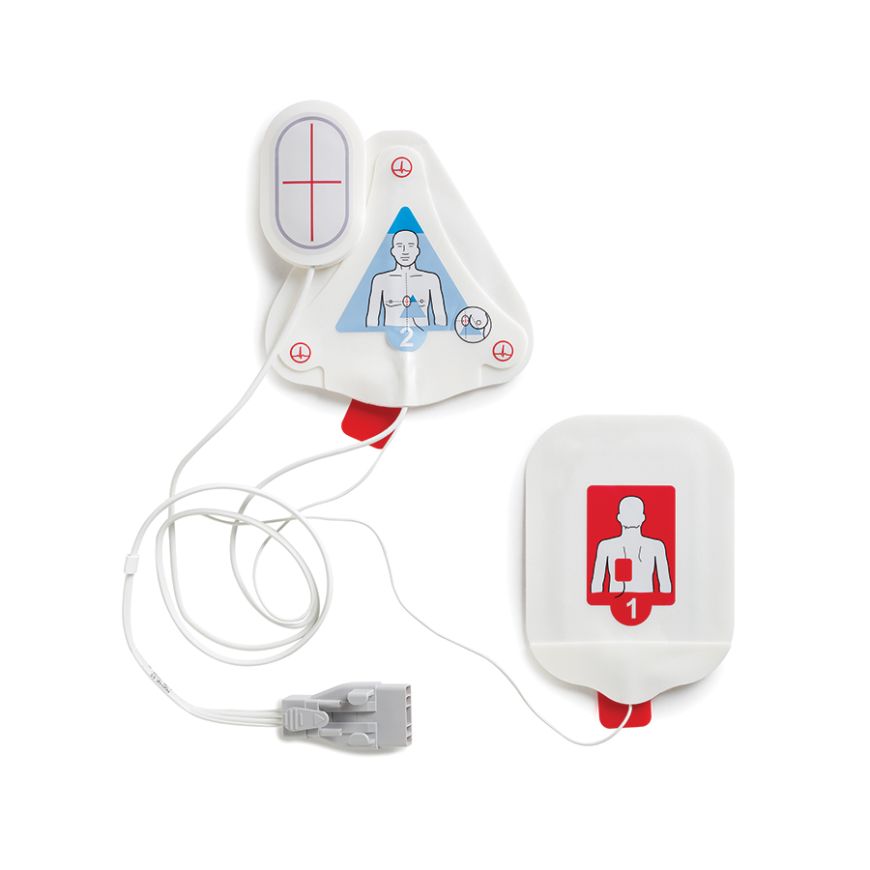
- OneStep Pads Connected to Defib Cable
- OneStep Pads (extra set)
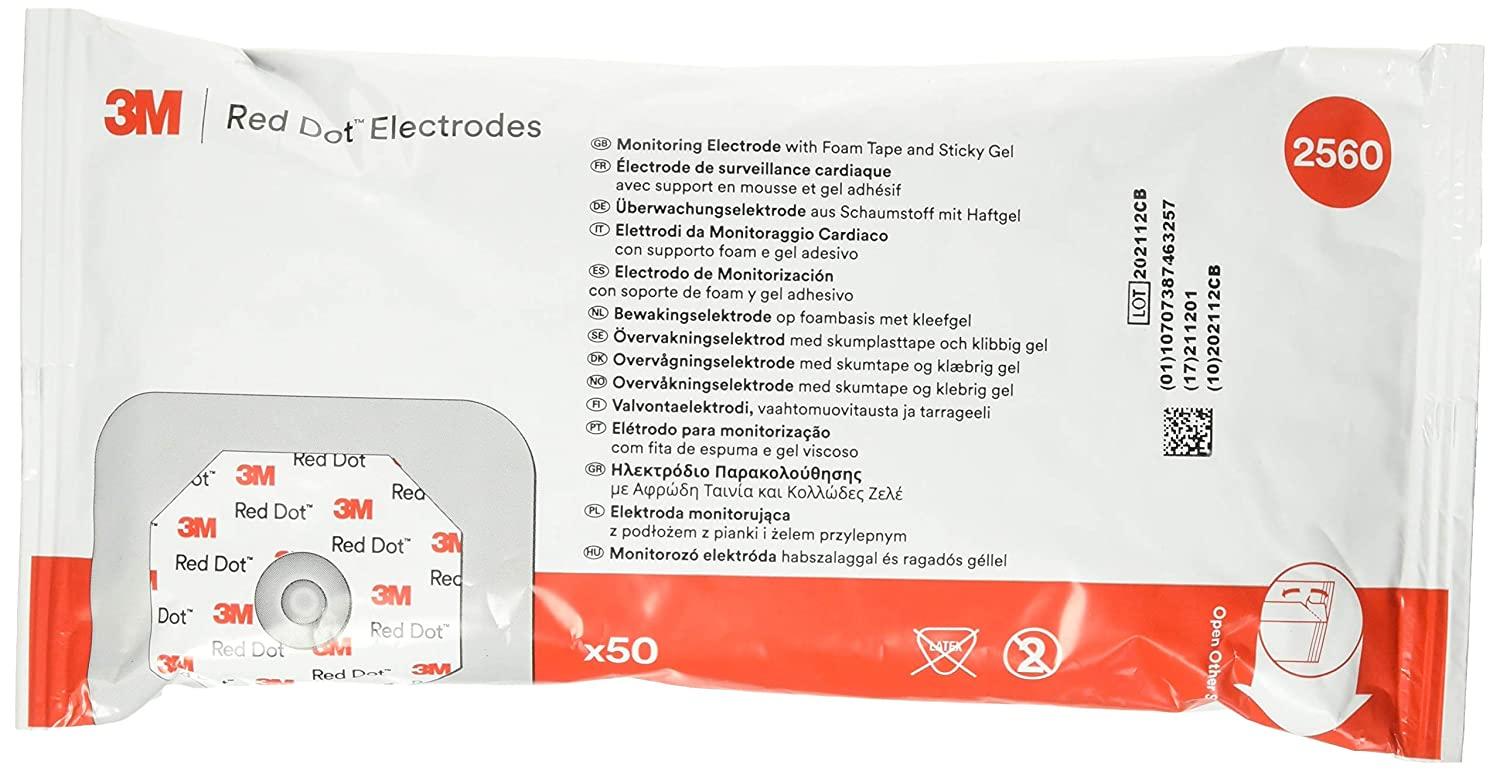
- Red Dot electrodes Pack x2
- Defib Paper
- Yankauer suction
- Suction tubing setup: Short Tubing 20 in
- Suction tubing setup: Long Tubing 12 feet
- Medium size gloves Box
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
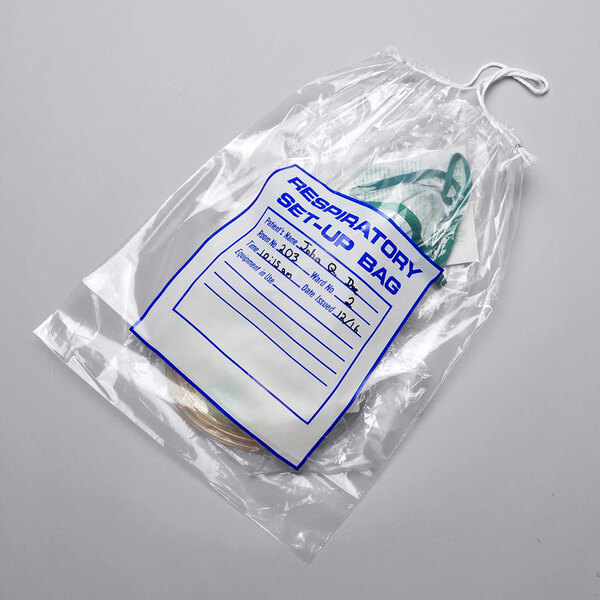
- Respiratory Supply BAG
- Respiratory Supply BAG SEALED
{kind=link}
- TOP OF CART
- Clip board with:
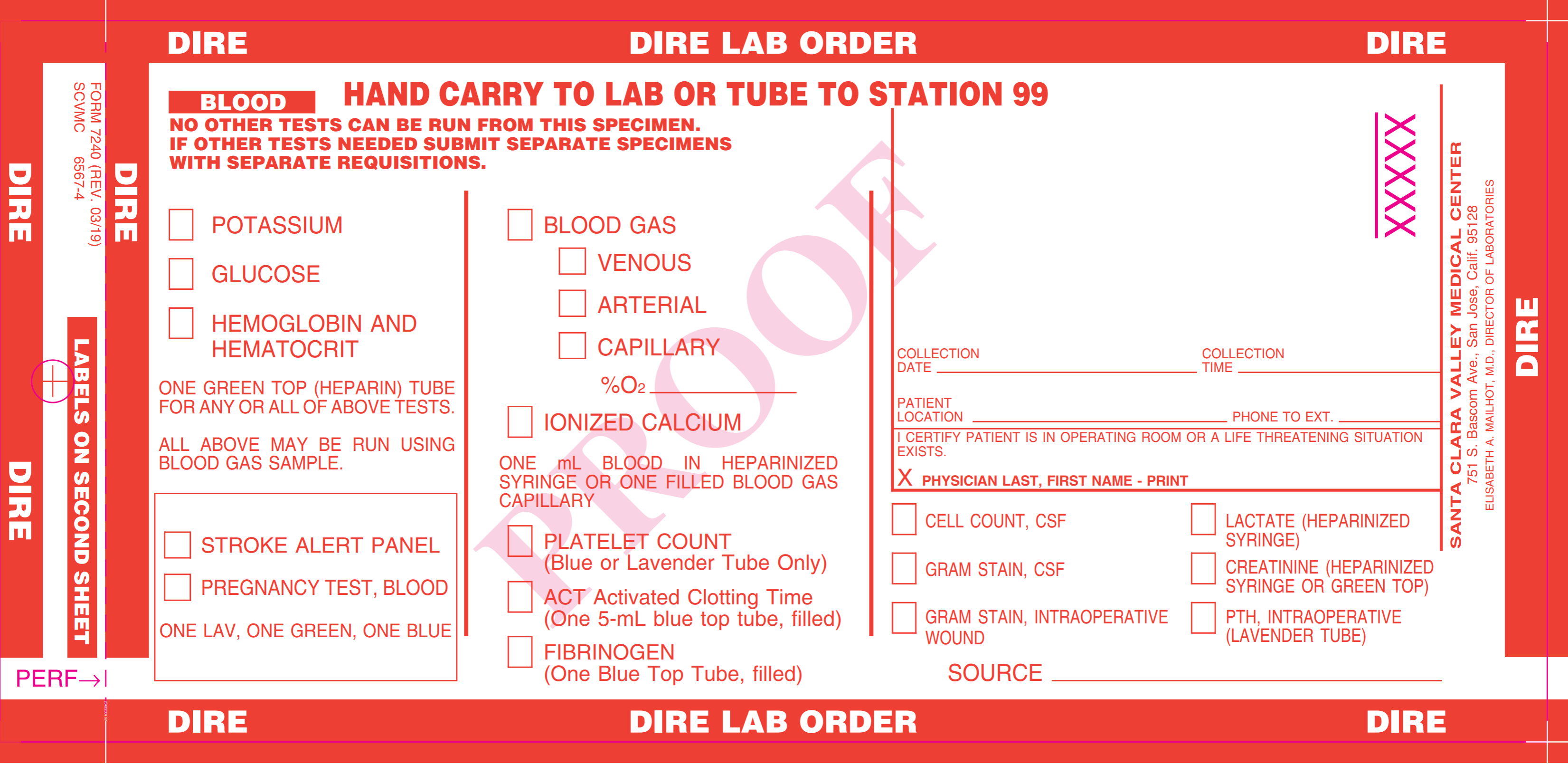
- Dire lab slips x4
- Code Blue Sheets x4
- Code Eval Sheets x4
- Red Lock for cart exchange
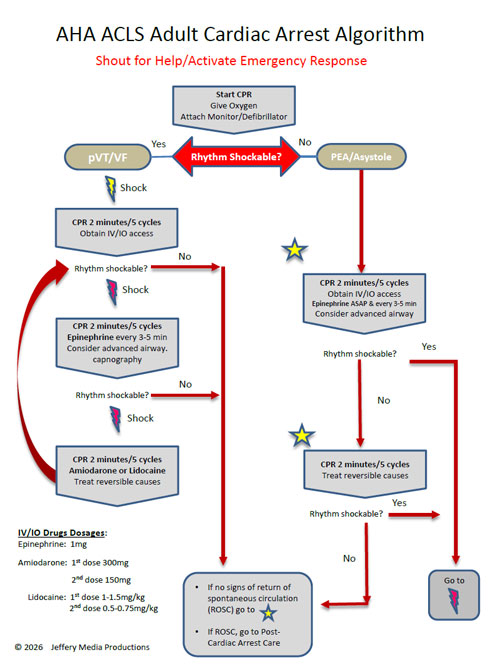
- ACLS Algorithm
- Emergency Manual on the cart (Yes/No)
- Defibrillator/Monitor
- Defibrillator/Monitor OneStep Cable
- Defibrillator/Monitor ECG Cables
- Defibrillator/Monitor NBP Cable
- Defibrillator/Monitor ETCO2 Cable
- Defibrillator/Monitor O2 Sat cable
- Portable suction Machine (Assemble the suction set up with short and long tubing → Ensure suction batteries are charging → Unplug & Test Suction setup for proper functioning → Plug the electrical cable after testing)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Defibrillator/Monitor Testing (Daily)
- Plugged into power outlet
- Gray power cord is connected to the black pigtail
- Battery light and AC power light green
- Green check mark is present in the display window
- Defibrillator/Monitor Testing (Every Tuesday)
- 30 Joule Defib Check
- Pacer Check
- Recorder Check
- SIDE OF CART
- Cardiac board
- Oxygen tank (full)
- Crash Cart Drawers
- Drawers 1-5 are Locked (Y/N)
- Crash cart Expiration date
- Lock number for Drawer 1-5: -DRAWER ONE- IV START- OGT/NGT - BP CUFFS, -DRAWER TWO- ART LINE SETUP, -DRAWER THREE- FLUSHES - IV FLUID SETS - MED, - DRAWER FOUR- Scalpel --CENTRAL LINE SETUP, DRAWER FIVE- TRACHEOSTOMY TRAY AIRWAY
- Emergency med module Exp Date
The standards is that for the crash cart, the daily checklist should be completed, no clutter on top, locked (including extra locks secured), and no expired medications or supplies noted
- DEFIB MONITOR:
- Plug it in and know chirping sound is a warning that not plugged in. Telemetry paper: where are extra roles CHANGE IF PINK RIBBON SHOWING. Use graph paper role, not blank role which is used for Central Monitor
- Know difference b/w how to use 3 leads vs. pads and when to use both.
- Quick Combo pads only for defibrillation. Practice AED function.
- Quick Combo plus 3 leads for cardioversion and pacing
- Know difference between Hands Off/AED vs. Hands On defib pads
- Red Dot leads, not blue tab 12 Lead EKG tabs
- Telemetry paper: where are extra rolls, CHANGE IF PINK RIBBON SHOWING, Use graph paper roll, not blank role which is used for Central Monitor.
- SUCTION:
- All 4 parts of suction should be together on top: Long tube, short tube, Yankuar and canister.
- Check if there is full, strong suction, if not, check for holes or cracks in blue lid.
- Suction machines are old and may not be holding charge, so unplug to check.
- Check connection b/w machine and suction canister, easily kinks off.
- Prepare to mount suction head into wall.
- Be mindful that suction/crash cart needs to be positioned near the head.
- AIRWAY BAG:
- Find O2 Flow meter, NRB and Ambu bag.
- Place bag at head of bed, so everyone can find it
- Ambu-bag mask gets easily lost when taking out of plastic bag.
- GRAB THE MASK and connect after taking off the white cap, Expand the Ambu
- If pt falls, assess situation. If C-spine concerns or not enough people to safely lift into bed, then leave on floor.
- If in chair, put pt back IN THE BED. Codes on the floor are poorly run. No room and more difficult to do everything.
- PRIORITIZE or ideally done all at once with team work: Check Pulse, Start CPR, Call for help, Place Pads, Back Board, Ventilate with Ambu, Check IV patency
- Roles of Code Blue Responders:
- Airway/Suction
- Pads/ Monitor/Defibrillator (Be prepared to shock with AED)
- CPR IV and Medications. (Be prepared to push EPI with a patent IV)
- Recorder. Mark the time that CPR began for the 2 min. pulse/rhythm check
- Code Leader.
- Good Quality CPR = Specific Body Mechanics
- Tall enough or use stool.
- Recognize if your chest or stomach get in the way. Shoulders over pts chest.
- Straight arms, strong wrists.
- Do you have stamina to do fast and hard for 2 minutes? 30:2. Count out loud.
- Continue CPR while defib monitor is charging, then clear.
- Excuse yourself, if you cannot provide effective compressions.
- Check carotid or femoral pulse for effective compressions and for 2 min. pulse/rhythm check.
- BLS or ACLS trained employees from the unit/department on which the Code Blue is located
- Calls Code Blue. Initiates BLS and AED team
- Gives report to Code Team Leader a) Length of time patient in arrest b) Events leading to arrest c) Patient history/diagnosis
- Documents events prior to Code Blue in the EMR.
- Makes available: Glucose meter, Portable monitor for BP for transport, 12 lead EKG.
- Clears out room of roommate, furniture
- Communicate with telemetry tech or REVIEW alarms prior to event and take rhythm strip to Code
- These are standards to abide by in general.
- All equipment on one side of the hall
- Nothing parked in hall longer than 30 minutes
- Top of linen cart covered; solid bottom on cart
- No open single-use vials; all discarded after use
- Opened multidose vials dated
- Pill crushers/splitters cleaned
- All doors/drawers locked when unused
- Opened multidose vials dated
- Discharged patient medications managed
- PoC Glucose monitors: Cleaned, controls and strips dated when opened.
- Call lights functional and within patient reach and alarms answered